
Placental tissue structure
Human placental tissue products can be comprised of different components of the placenta, such as the amnion, chorion and umbilical cord, in various combinations and quantities. The grafts are biocompatible and degrade in time.
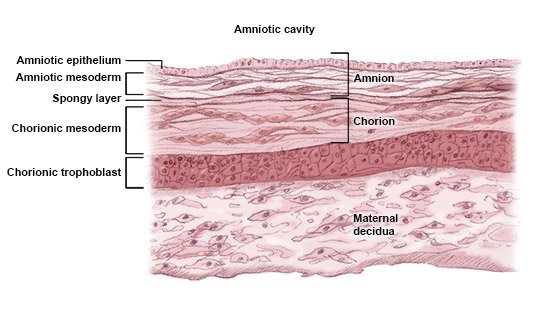
Amnion
The amnion is 50-100μm in depth and composed of a single-layered epithelium and the amniotic mesenchyme. This is the layer of tissue that lies closest to the fetus. It contains epithelial cells, fibroblasts, MSCs and macrophages.
Chorion
The chorionic membrane is composed of fibroblasts and trophoblasts and is connected through the maternal decidua. It also contains MSCs and macrophages.
The chorion and amnion can be easily separated and have therapeutic uses alone or in combination; however, the trophoblast layer can cause an immune response. These allografts have applications across a wide range of therapy areas.
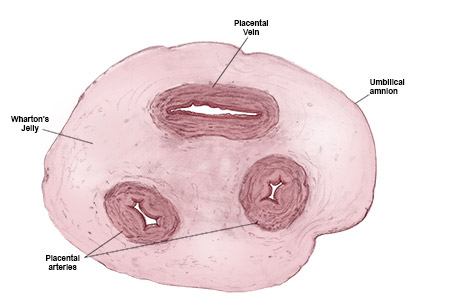
Umbilical cord
The umbilical cord is stronger and thicker than amnion and chorion, covered in amniotic epithelium and contains two arteries and a vein immersed in Wharton’s Jelly (containing fibroblasts, MSCs and hyaluronic acid). Umbilical cord allografts can be applied in surgical settings as a covering or wrap in procedures, such as tendon repairs.

It also has low immunogenicity
Compared with other transplanted tissues, human placental tissue has low immunogenicity and therefore has a low risk of immune reactions and rejection. Several clinical studies have shown that allogeneic transplantation of the amniotic membrane does not induce acute immune rejection in the absence of immunosuppressive treatments.
This feature is associated with the low or limited surface expression of HLA class II (HLA-DR) and costimulatory molecules responsible for T cell activation. Immune tolerance is also mediated by active immunosuppressive properties of the tissue from the secretion of molecules, such as HLA-G, B7-H3, PD-L1 and PD-L2.
- Kubo M, Sonoda Y, Muramatsu R, Usui M. Immunogenicity of human amniotic membrane experimental xenotransplantation. Invest Ophthalmol Vis Sci. 2001;42(7):1539–1546.
- Magatti M, Vertua E, Cargoni A, Silini A, Parolini O. The immunomodulatory properties of amniotic cells: The two sides of the coin. Cell Transplant. 2018;27(1):31–44.
- Nikjaed H, Habibollah P, Jorjani M, Ahmadiani A, Ghanavi J, Seifalian AM. Properties of the amniotic membrane for potential use in tissue engineering. Eur Cell Mater. 2008;15:88–99.
- Silini AR, Cargnoni A, Magatti M, Pianta S, Parolini O. The long path of human placenta and its derivatives, in regeneration medicine. Front Bioeng Biotechnol. 2015;3:162.
- Banerjee J, Dhall S. Therapeutic benefits of treating chronic diabetic wounds with placental membrane allografts. In: Bagchi D, Das A, Roy S, eds. Wound Healing, Tissue Repair and Regeneration. Academic Press, Cambridge, MA, USA 2020:323–335.
- Brantley JN, Verla TD. Use of placental membranes for the treatment of chronic diabetic foot ulcers. Adv Wound Care. 2015;4(9):545–559.
- Mamede AC, Carvalho MJ, Abrantes AM, et al. Amniotic membrane: from structure and functions to clinical applications. Cell Tissue Res. 2012;349:447–458.
- Wang HS, Hung SC, Peng ST, et al. Mesenchymal stem cells in the Wharton’s jelly of the human umbilical cord. Stem Cells. 2004;22(7):1330–1337.